Last update | February- 15th 2026

CASE EXAMPLES RELATED TO OUR APPROACH TO CLASSICAL & DIGITAl DENTISTRY - QUALITY WITH CONSISTENCY
These images are accompanied by technical support which maybe useful to student dentists and the inexperienced dentist and dental technicians wishing to improve there skills.

Case No.001; A RECONSTRUCTION - HOW WE MADE IT

This young ladies smile said it all. This case did not require any complex color matching but it needed a geometric reconstruction. The original dentition was dysfunctional the mandible was displaced and the dentition had a high degree of attrition and had an open posterior occlusion which was driven also from a fulcrum point. Its a typical scenario when the mandible has no place to retreat to. The solution was to deprogram the muscles and reposition the mandible back into Cr.
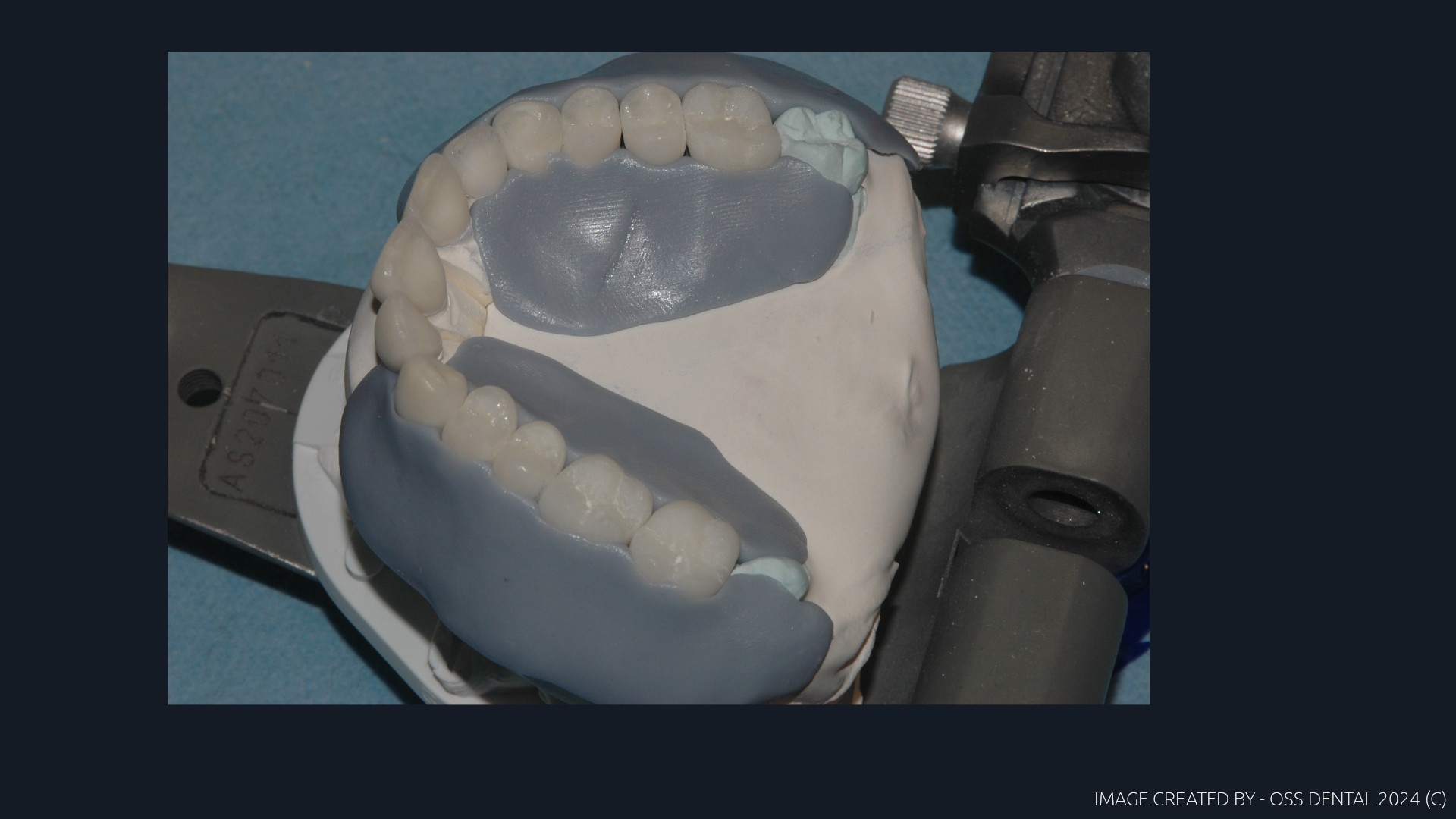
This corrected the arc-of-closure and allowed us to establish a correct guidance that was tuned correctly to that patient by three simple associations. By doing that the mandible then could once again become a Class III lever. The case was mounted by a facebow, with a centric bite and a protrusive bite provided by a dentist. To access the condylar width we use photography to determine the intecondylar distance to set the cuspal positions by tracking the medial movements. No need for anything else, this then was a simple technique to configure the correct case result and the vertical was not changed either. By suggesting mixing Emax for the anteriors and four Zr units to stabilized the posterior segments we agreed this as the best combo for this case as form changes were required and a stable occlusal table needed to be created to complete the treatment.
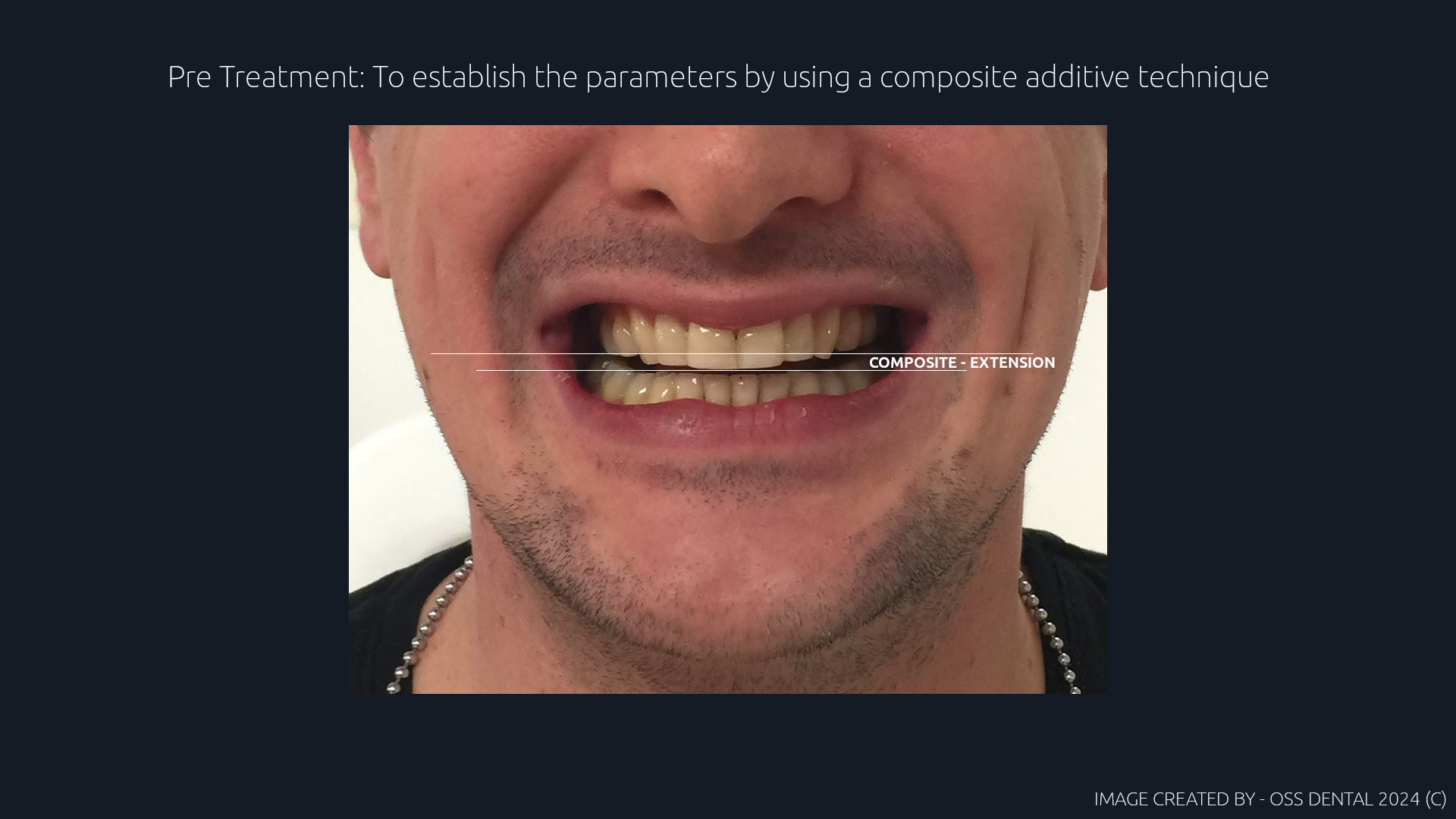
No monolithic units were used, the ceramic was full coverage so shock resilient absorption was correctly spread across the entire arch by using one specific ceramic material which was IPS Emax over lithium and zirconia. The case then made no offensive noise either as Emax is a softer more resilient ceramic, but it needs to be protected and that can be achieved by using posterior Zr to stop compression and the anterior guidance takes care of the medial translated loadings by using the disclusion formula of 2-2-1. Cuspal clearances could now function correctly and the arc of closure was now no longer antagonistic and the attrition stopped and comfort returned. Pre-design and components were made digitally. Temps confirmed the concept and the lower incisors were corrected with composite to complete the guidance. The rest was feel and touch by a team who had experience and knowledge.

A final look
Case No.002; FRACTURED DENTITION - HOW WE MADE IT

This was a simple case made as two single PFM units. The injury was due to a skate board incident. The reason to use high content gold alloy was the palatal aspect needed to match the concavity of the palatal aspect to maintain the original anterior guidance, the gold acts in the same way as the natural attrition of enamel as it will wear in a similar way. Gold content was 80%. The models were mounted by a facebow to get the correct occlusal inclination. Condyle inclination was not required as the anteriors could be medially tracked using a Stuart articulator. The final and most difficult part to finalize this case was to match the exact texture of the existing anterior surfacing as this patient was young. That was done by hand ceramic scraping and texturing with carborundum paste, not diamond paste.